

By Rosalie Mattiola
Abstract
Research Question: How has the mapuche medical system adapted or modernized regarding the treatment of modern diseases like diabetes, cancer, and/or hypertension, and what is the effect on patient well-being?
Objectives
- To characterize the process of modernization/adaptation of medical treatments amongst the mapuche.
- To explore the medical hybridization or medical pluralism amongst the traditional and biomedical health systems regarding the treatment of modern diseases.
Background
The mortality rate for modern diseases has rapidly increased in Chile over the last decade. It has been shown that these diseases burden the mapuche community more than the non-mapuche community (Pedero Sanhue, 2011). The mapuche represent the largest population of indigenous peoples in Chile. They have suffered long-term cultural discrimination and their medical system has been subjugated although it is widely utilized.
Methodology
A total of 27 surveys were gathered from patients in waiting rooms at 2 community health care centers in the towns of Makewe and Puerto Saavedra in La Araucanía, Chile. A total of 12 interviews were collected from health professionals, mapuche leaders, citizens and governmental workers. The data was collected during 2 weeks in May of 2017.
Results and Conclusions
Some patients prefer to use both mapuche medicine and biomedicine for treatment of their chronic, non-transmissible disease. Both mapuche and non-mapuche patients utilize mapuche medicine. The specific treatment methods have not changed in order to treat modern diseases. However, the mapuche medical system has adapted in its interaction with the biomedical system. The most apparent change is the use of machis in health centers. Furthermore, medical pluralism is widespread although medical hybridity is not.
Recognition
I’d like to thank all those involved in the preparation, the planning and the execution of the project. I received plenty of assistance in skill and idea development and am endlessly grateful. Thank you to:
- My advisor for transmitting his experienced-based knowledge of anthropological studies, his guidance, his reassurance and for conveying his friendly, charismatic, and energetic spirit. I wish him and his new family the best in the future.
- The SIT Program Directors for their lessons on project development and suggestions for improvement. Their hard work is recognized and appreciated.
- The directors and staff of the health centers in Makewe and Puerto Saavedra for welcoming me into their workplace and for their patience in working with a U.S. American student.
- The informants for their time and their patience. This project would not be possible without their willingness to share their experiences and opinions.
- My host families for their generosity in providing me with a comfortable environment to live, learn, eat and work.
- My parents for giving me this opportunity to travel and study abroad and for their support throughout the semester and always.
- Sarah and Maya for their friendship, aid, advice, stimulating conversations and for keeping me cheerful during the ISP period.
- SIT World Learning for their time spent planning and enhancing the international study programs.
- The entire community of La Araucanía for treating me well and sharing their culture.
Introduction
Mortality
Between 1997 and 2013, Chile experienced a shift in mortality rates of diseases considered “modern” or “western” like cancer, diabetes and cardiovascular disease. The number of deaths caused by malignant tumors of the colon, sigmoid, rectum, anus, liver, pancreas, trachea, bronchus, lung, head, lymphatic tissues, hypertensive disease, cardiac arrhythmias, arteriosclerosis, aneurisms, and aortic dissections have dramatically increased in the last two decades. Within 16 years, the number of deaths from cancer of the colon, sigmoid, rectum, anus, pancreas, trachea, bronchus, lung, and head have more than doubled. Those caused by hypertension jumped from 1,700 in 1997 to 4,574 in 2013. Moreover, the number of deaths from cardiac arrhythmia more than tripled in this time (DIES-MINSAL Series Principales causas de muerte tasas según sexo Chile).
In the region of Araucania, where the highest percentage of indigenous peoples reside (Johnson 2017), the mortality rates for malignant tumors increased from 123.1 to 153.2 deaths per 100,000 habitants over the period of 2000 to 2011 and that of hypertensive diseases increased from 12.5 to 20.7 deaths per 100,000 inhabitants (DIES-MINSAL Series 11- Araucania). The death rate from diabetes remained level but the UN Report on the Health Status of the World’s Indigenous Populations highlighted alarming rates of diabetes: “Worldwide over half of indigenous adults over 35 have type II diabetes. These numbers are expected to increase. In some indigenous communities, diabetes has reached epidemic proportions and has threatened the very existence of the community” (Muñoz 2016).
Within Araucania, it has been found that indigenous inhabitants are subject to higher mortality rates for the same diseases than compared to the non-indigenous Chilean citizens. The Ministerio de Salud (Ministry of Health) presents data showing the mapuche indigenous population to have a 60% higher risk of dying from illnesses of the circulatory system than non-mapuches (Pedero Sanhue 2011).
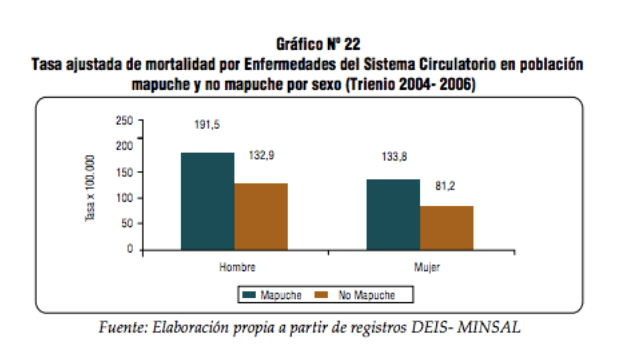
Mapuches in urban settings almost always have a much higher mortality rate than those in rural areas (Pedero Sanhue 2011). The same concept holds true for mortality by cerebrovascular disease and cancer, although the mapuche burden of cancer mortality is stronger amongst females than males.
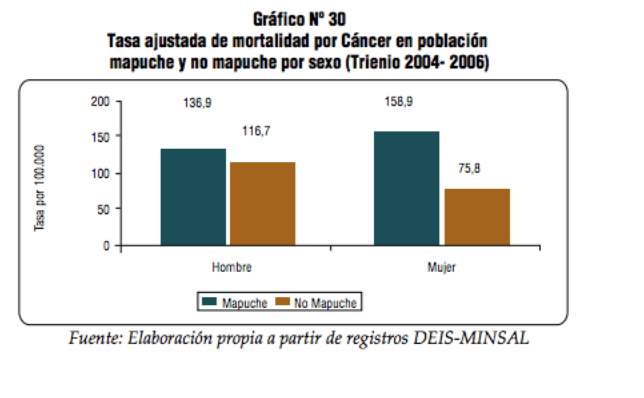
The mortality rate of cancer of the digestive organs in mapuche women is especially alarming.
Modernity
The appearance of the aforementioned modern diseases amongst Chileans and mapuches can be associated with modernization over the last three decades. Muñoz defines the concept, citing Bengoa (1996:7): “Modernization, understood as the uncritical adoption of norms, behaviors, and products coming from “developed” countries, is now a universal reality” (2016). New lifestyles, diseases, systems of health care and treatment methods have mixed within the indigenous culture. A common trait of modernization of indigenous communities is the increased vulnerability to “modern” diseases, which is widely affected by social determinants of health (Montenegro 2006). Linking modernization to urbanization and transfer of knowledge, Torri explains, “with the process of increasing assimilation to the dominant Chilean culture following immigration into urban areas, the Mapuche are exposed to new concepts when chronic illnesses, such as cancer, stroke and diabetes, are diagnosed by biomedical practitioners” (2011). The diseases diagnosed by biomedical practitioners are then interpreted, rationalized and treated by the mapuches. A study from Muñoz found that “All users identified diabetes and hypertension as diseases ‘that we didn’t have previously.’ They attributed these diseases to the consumption of processed foods with high fat and sugar content and associate these foods with a modern lifestyle” (2016). Therefore, modernity has had a visible effect on the health of the indigenous.
It is important to note that the labeling of ideas and concepts as “modern” forces the presence of the opposing label “unmodern.” The current hegemonic system assigns value to the concept “modern” and undermines all things “pre-modern” (Awah 2008). This project attempts to avoid this designation of “better” or “worse” associated with modernity. When methods and beliefs adapt, it is not because they are seeking to become more modern and thus better, rather that they change to meet the need of the community. This change is inevitable when confronted with modernization. “Modern” and “pre-modern” concepts cross and interact. Modern diseases are not only knowable by modern medicine—it is permissible and acceptable for modern diseases to be treated by unmodern medicine (Awah 2008). This is precisely what this investigation seeks to study—the intersection of modern and unmodern and the adaptation of practices based on the transmission of knowledge.
Medical Adaptation
Change occurs within many medical systems and is particularly visible among indigenous cultures. Torri notes, “One aspect of indigenous culture that has undergone considerable change is the system of traditional medicine, i.e. the health knowledge, beliefs, values, skills and practices of indigenous people, including all clinical and non-clinical activities and institutions that relate to the health needs of the people” (2011). Acculturation via modernization provides an opportunity for role adaptation, whether that creates a beneficial or harmful situation (ibid.). Previous research has studied the specific adaptive role of machis (traditional mapuche healers), initiated by modernization and the desire to meet the need of their community. A study correlated the new capitalist system and the notion of modernity with the types of illnesses that machis treat and concluded that “the role of the machi in the 20th century is different enough from that of the 19th century” (Bacigalupo 1993). Adaptation supported the survival of their livelihood as healers and has allowed the role of the machi to outlast many other Mapuche authorities (Torri 2011). A historical holistic patient-centered focus catalyzed machi practical adjustment; “The machis have had to adapt to the demands of their patients” (Bacigalupo 1993). The need to study adaptation as an important factor in reducing morbidity is summarized by Torri:
The various ways in which healers, for example, have altered or are adapting their training, therapy and organization to meet current sociocultural, economic and political changes need to be investigated. It is important to study the different processes of change in the curative, preventive and sociopolitical roles of traditional medical practitioners. …Changes occurring in the practice of traditional medicine need to be explored, especially if the World Health Organization’s recent proposal that traditional medical practitioners should be involved in National Health Planning and Health Care Delivery Systems is to be assessed realistically. Knowledge of the nature and direction of the transformations occurring in mapuche traditional medicine is also required to enable health planners to decide how traditional health resources could be mobilized to reduce the rates of morbidity among indigenous people in Chile as well as other Latin American countries (2011).
Justification
Studying local understandings, perceptions, and treatment methods is essential as the prevalence and mortality rates of modern diseases increase. The concepts of modernity and adaptation are especially relevant to this study and to others that seek to conceptualize current indigenous norms. Finally, appreciating indigenous medicine should be of utmost importance, rather than being ignored or discredited. The World Health Organization estimates that 3.5 billion people in the developing world depend on traditional medicine for their primary care (Torri 2013). Even in Chile, an economically developed country, “non-biomedical healing systems continue to attract substantial numbers of patients,” regardless of the “enormous structural power and professional sovereignty that biomedicine has achieved” (Torri 2011).
Investigation Theme
This study seeks to investigate the process of adaptation of traditional mapuche treatment methods for modern or occidental diseases like diabetes, cancer, and/or cardiovascular diseases and its effect on the conditions of well-being. The goals of the investigation are to showcase the reality of the complexity of health care, to create a referential resource for the improvement of pluralist medical treatment for modern diseases, and to highlight the importance of non-biomedical methods, hereby referred to as self-care. This is an exploratory,descriptive, and prospective qualitative study. It was completed over a one-month investigation period in the southern region of Araucanía, Chile in May 2017. The project consists of interviews with mapuche leaders or medical professionals and surveys with mapuche citizens and medical system users.
Objectives
General Objectives
- To characterize the process of modernization/adaptation of medical treatments among the mapuche.
- To explore medical hybridization or pluralism between traditional and biomedical health systems with respect to the treatment of modern diseases.
Specific Objectives
1a. To understand how the traditional treatments were developed for non-transmittable chronic diseases like those defined by we kutran and wingka kutran.
1b. To identify and comprehend why treatment methods for modern diseases developed within the traditional mapuche medical system.
2a. To conceptualize the perceptions of the indigenous peoples regarding the treatment of modern diseases.
2b. To identify how modern diseases are recognized, interpreted and treated by mapuche individuals through traditional indigenous practices.
2c. To obtain and evaluate perceptions and preferences regarding treatment of modern diseases via the various medical systems (traditional, occidental or other).
Theoretical Framework
Historical Framework
As disease prevalence changes over time, one would expect the treatment styles to adapt in accordance with the health/disease/care principle developed by Menéndez which proposes that subjects elaborate their ailment which determines the types of care they search for (2005). For the mapuche, this process of adaptation has been occurring not only in their health care environment, but also throughout their history of conflict with the Chilean state. In the late 1800s the Chilean state began the Pacification of the Araucania, a euphemism for mapuche genocide, deculturation, and territory loss. From then on, they have lived the struggle of modernization, adaptation, hybridization, identity loss, and discrimination.
Cultural Framework
The mapuche represent the largest population of indigenous peoples in Chile, accounting for 84.11% of the indigenous population, according to the 2012 census (Johnson 2016). Their moral values are guided by the belief in their sacred ancestral spirits (Colicoy 2017). For this reason, their connection to land and nature—their waj mapu—is also very strong (Pichinao 2003).
Health Framework
Their health beliefs are centered on the concept of equilibrium between human beings, ancestral spirits and the other beings of waj mapu. When an individual infringes upon the norms of the mapuche universe, they can become sick (Pichinao 2003). The mapuche notions of health and illness are distinct from western beliefs. The abstract concepts of health and disease are replaced by the opposition of küme felen and weza felen. Küme felen is the entirety of well-being and good living. This includes emotional, physical, spiritual, economic, political, environmental, and familial well-being. Weza felen is poor being, when one realizes that they are psychologically, socially, biologically, culturally or spiritually in disequilibrium. A study from Muñoz found that the mapuche medical system understands disease to occur when “individuals violate the laws and norms that maintain harmony and balance between the earth (ad mapu, the law of the earth) and society (ad che, human law), and also when individuals neglect traditional cultural practices (2015).” Thus, their perception of health is a process, not a state, since it is linked to many other social phenonema (Cuyul, Caniullan 2017). According to Pichinao, mapuches believe that “disease is not only a biological or physical state, rather disease is always moral and social. Diseases are formed from a socio-spiritual disequilibrium.”
Pain, the tangible aspect of disease, is referred to as kutran. The mapuche classify various types of pain according to the origin or believed cause. Two classifications of special interest are we kutran and wingka kutran. We Kutran are understood as new illnesses (we = new) some brought from European colonizers (wingka) but have been named and recognized by the mapuche healers. For example, diabetes is kowi mollfüñy and cancerous tumors are kotipaw. Wingka kutran are disease of modernity and urbanization directly correlated with the presence of non-indigenous colonizers. These diseases like Auto-Immune Deficiency Syndrome (AIDS) and depression are not incorporated or named within the mapuche health system, but they can still affect the mapuche population (Caniullan 2017).
The appearance of new diseases brought about the need to treat them within the mapuche health system. Some of the commonly used traditional methods were applied and altered to treat we kutran and wingka kutran. The mapuche healers called machis typically use herbal and spiritual methods like prayer, singing and playing the kultrun drum, as well as diagnosing illness by observing urine or clothing (Torri 2013). Machis attempt to treat the person and not only the disease (Muñoz 2016). Another type of mapuche healer called a lawentuchefe uses exclusively herbs to treat usually simple ailments. The following herbs are said to treat some of these modern diseases such as diabetes, cancer and poor circulation: boldo (foldo), canelo (foye), hierba del clavo (llante), hualtata (waltata), llareta (leliantü), quintral (kintral), palo negro (kudü negro) (Caniullan 2017). A 2015 study on the chemical composition of palo negro even confirmed its anticancer properties by identifying its ability to decrease cell viability of cancer cell lines (Bosio 2015).
Recently, machis have been hired by the occidental and governmental health centers in an effort to adhere to the principles established by the Special Program for Indigenous Peoples (Spanish acronym PESPI) and the Indigenous Law 20.584, which requires health care centers to provide culturally pertinent health care to indigenous users if desired (Cuyul 2017). This seemingly beneficial step towards interculturality is in reality, superficial at best. The burdens outweigh the benefits in this case. Although the machis and mapuche curers may be more centralized and accessible, the relationship between cultural healers and occidental doctors is rarely free of power struggle and cultural misunderstanding. The biggest misunderstanding of all may be the fallacy that any given machi can practice their treatment in any setting without consequences on the strength or effectiveness of their treatments. Torri explains the finding that, “machis must pray to their spirit and ask permission of the rewe (spirit figure) when they want to leave the house. It is believed that they become sick if they violate the rules that are considered appropriate for the machi, or when they are absent from their homes for long periods of time” (2011). Some attempts at interculturality seem to instead incentivize culturally inappropriate, non-ancestral situations. Thus, interculturality at its best could in fact be considered multiculturality or medical pluralism where users are empowered with the freedom to choose the type of health care they desire without barriers of stigma, accessibility or financial struggle.
It is important to note that health care is complicated, just like many other aspects of life. Although we all experience disease and discomfort, each culture has its own approaches and preferences to curing what ails its people (Muñoz 2016). The techniques vary even within a single culture. Not all machis practice the same methods—there is no machi “school” or standardized exams (Cuyul 2017). A study from Bacigalupo concludes, “machis are not a uniform group although they have certain generalized characteristics that group them under this term. The various forms taken by machi are related to their geographical location, the practice of intensive agriculture and the cult of fertility, the proximity to urban centers and the existence of ritual leaders. It also influences their degree of adaptability to the processes of acculturation, and their type of appeal and reputation in the community” (1993). Therefore, the mapuche health care world is also complicated by the influence of personal preferences and the interaction with modernity.
Conceptual Framework
The authority figures of the Mapuche community are the lonkos and the health agents. A lonko is a community leader who tries to represent the opinions of the community and improve their daily cultural situation. They are typically older men who are democratically elected because of their ability to articulate knowledge well. A machi is a health agent who tries to cleanse a person of disease, whether it is of spiritual causation or not. They diagnose through reading or viewing urine because “the urine knows.” Sometimes a clothing item can also be used to diagnose disease. A machi can perform a machitun, a spiritual ceremony to “wash the body,” involving many people. They can also treat with herbal medicines in the form of infusions or teas, sometimes called simply, “liquids.” Another mapuche health agent is a lawentuchefe who has the knowledge of lawen or herbal remedies. Like the machis, they use herbal infusions for treatment. Both machis and lawentuchefes have a spiritual gift through which they received their knowledge of healing.
To conclude, the mapuche world, like other indigenous communities, has experienced high interaction with the modernized world, but its traditional patterns are still valued. This study tries to understand if this concept applies to the mapuche medicine system as well.
Methods
Data for this exploratory, qualitative study was gathered between May 7 and May 20, 2017 in four areas in the region of Araucania, Chile. Interviews were collected in the city of Temuco at the Universidad de la Frontera, and the towns of Cajón, Makewe and Puerto Saavedra. Surveys were administered in the waiting rooms of the Hospital Makewe and the Mapuche Health Center in Puerto Saavedra, and in the town plaza of Puerto Saavedra.
A total of 27 surveys were obtained. When approaching possible participants, the investigator gave a straightforward introduction identifying her intent and theme of study before asking permission to ask questions. The participants were assured that anonymity would be maintained and that they were not required to answer any or all of the questions. Rejections from participants were fully accepted. To obtain the data, the investigator read the survey questions to the participant and recorded the information while the participant answered or immediately after the conversation ended.
Permission to survey patients in the waiting room from the respective director and coordinator at both Hospital Makewe and Mapuche Health Center in Puerto Saavedra was obtained before data was collected. The amount and type of questions asked from the survey was determined by the participant’s ability to hear and understand, ability to respond appropriately, and interest in providing information. Questions were restricted based on cultural pertinence and time available before the participant was called into the health care provider’s office. The surveys collected in the plaza of Puerto Saavedra were regulated similarly. The survey was adapted several times. As data was collected, impertinent or inadequate questions were removed and/or replaced.
A total of 12 interviews were administered. The interviewees gave written or verbal informed consent to participate. The questions of these semi-structured interviews were categorized for “professionals,” for “citizens” or for machis. All 3 sets of questions can be found in the appendix.
The investigator chose questions based on the order of topics in the conversation, the specialization of the interviewee, and the perceived effectiveness of the questions. If needed, the interview was shortened for time restrictions and adapted as questions were rearranged, removed and/or replaced. Unstructured questions were added to achieve depth of conversation.
The 10 “professionals” interviewed are defined as those who work within the healthcare field, are involved in a governmental organization or act as authority figures within the mapuche community. One machi was interviewed. The one interviewee considered a “citizen” was not classified as a machi and does not have the “professional” criteria described above. All 12 interviewees admitted that they felt like part of the mapuche community although 11 interviewees were of mapuche descent, and 1 was of Spanish decent but has spent 12 years working with the mapuche community. Eight males and 4 females were interviewed. These 12 interviewees consisted of 2 social workers, 1 lawentuchefe, 1 intercultural facilitator, 1 coordinator of a mapuche health center, 1 governmental employee of the Program for the Development of Indigenous Territory (Spanish acronym PDTI), 3 lonkos, 1 machi, 1 artisanal vendor, and 1 anthropologist and government program director.
These contacts were established via convenience sample and snowball effect. The 4 primary contacts were pre-established through SIT, and presented 2 secondary contacts, who presented 2 tertiary contacts. The other 4 interviewees were contacted through a homestay family friend, a spouse of an interviewee, an author of a cited investigation, and via survey. Two of the 12 interviewees taught a class for SIT during the travel period, 2 were met twice before via the town investigations, 1 was met only once before, and 7 had no formed a priori relationship, but rather were simply secondary contacts provided by primary contacts.
An iphone voice recorder app was used to record the interviews once permission was granted. If the interviewees felt uncomfortable being recorded, the key phrases from the interview were written. Pertinent information was transcribed as closely to word-for-word as possible. Key phrases were then extracted from the Word document into Excel and categorized by theme.
Results
Surveys
A total of 27 surveys were collected. Fourteen were completed in the waiting room of Hospital Makewe and 15 in Puerto Saavedra. Male participants represent 63% (n=17) of the data while females constitute 37% (n=10) of the data. Participants were selected from the adult population; one was 21-30 years old, three were 31-40 years old, four were 41-50 years old, five were 51-60 years old, nine were 61-70 years old, four were 71-80 years old and one had an unidentified age.
The data presented 55% (n=15) of participants diagnosed with a “modern disease” like diabetes, hypertension, or cancer.
Of the 15 participants with a “modern disease,” 11 identified as mapuche and 4 identified as non-mapuche. Being of mapuche descent did not determine their use of the mapuche medical system. Both mapuche and non-mapuche individuals admitted to using mapuche medicine.
Regarding the type of health care professional the participants with a modern disease see for treatment, 6 exclusively see a doctor, 6 see a doctor and/or a machi, 1 sees a doctor and/or lawentuchefe, 1 sees a doctor, machi, and/or lawentuchefe, and 1 sees a doctor, physical therapist, machi and/or lawentuchefe.
When asked if mapuche medicine is used to complement biomedicine, 5 participants with a “modern disease” responded that mapuche medicine is principle, in other words not “alternative” or “complementary.” Two felt that mapuche medicine is used to complement biomedicine (wingka medicine). Two responded that they do not use western biomedicine at all, and one responded that they do not use mapuche medicine at all, so biomedicine is their principal form of treatment.
When asked which types of treatments they use, participants with modern disease responded with great variety. Three use occidental treatments (pills) only, one uses mapuche treatments only (herbal medicine or spiritual ceremonies), 5 use both occidental and mapuche treatments, 1 uses occidental treatment and home remedies, 1 uses mapuche treatments and home remedies, 2 uses all three types of treatments and 1 uses non-mapuche herbs (medical marijuana).
Interviews
The mapuche cultural health system is based on holistic, integral treatment. Diseases, especially modern diseases, are not understood as isolated problems that can be solved with a discrete treatment like a pill or an herb. Rather, since mapuche healers understand the entire body, mind and spirit to be linked, their treatments attempt to get to the root of the cause, whether that be inflammation of spiritual loss or transgression. Their treatments claim to also incorporate the social aspects that the biomedical system is lacking.
“Because often, although one is on biomedical treatment, the biomedical method does not do the job integrally. It always lacks something. We understand that diseases can have a component principally but not absolutely physical or biological. Our logic is always on the spiritual level, on the social level, on the psychological level, and biomedicine does not work on these levels.”– An anthropologist
Moreover, a social worker noted that treatment of modern diseases specifically require consideration of the family life, work life and the community atmosphere. Because the biomedical system frequently does not consider these factors and is sometimes unsatisfactory, patients are seeking “alternative” treatments. Those may be traditional medicine, religious therapy, Chinese medicine, homeopathy, or home herbal remedies (Sergio Bermudo Muñoz, personal communication, May 18, 2017). According to an intercultural facilitator, people are searching for the most natural, and the least damaging remedies. The mapuche in particular are looking for medicine that is their own, but may not be recognized within the formal system. It is apparent that people who are sick are not thinking about the hegemonic system between biomedicine and “alternative,” “complementary” or “indigenous” medicine. Rather, they are merely seeking out the best possible manner in which to improve their health, whether that be with pills, herbs, spiritual ceremonies, or acupuncture.
“Suddenly people are much more intercultural than [health professionals] ourselves. They alone seek, deliver, talk, pass data to each other, travel. The people do not want to conform with the systems of care, rather the treatments.” –Sergio Bermudo Muñoz
Therefore, when accessible and available, mapuche freely choose a treatment method based on their own values and beliefs. Mapuche medicine is elected as a treatment method for modern diseases because it is considered less invasive, more prolonged, less destructive, and free of side-effects or contraindications with other medications. Moreover, it is sometimes chosen after the biomedical system proves unsatisfactory. For this reason, the non-mapuche population is trying mapuche medicine. A lonko explained that this is completely acceptable because mapuche medicine responds to human beings in general, not only mapuche people. The non-mapuche patients may prefer mapuche medicine because the machi or lawentuchefe looks into their eyes, takes their time, and establishes a personal connection.
“In reality the mapuche medicinal treatment is personal. That is to say a machi or lawentuchefe makes his or her therapeutic preparations according to the personal characteristics of each person. And this is one of the differences with our western system. The difference with mapuche medicine is that it is made for the person more than for the disease. So the lawentuchefe or the machi established a very close, very private link with the patient.” –Sergio Bermudo Muñoz
Some patients chose the natural treatment for fear of high chemical ingestion that is prescribed in the form of pills from biomedical doctors. An artisanal vendor explained her reason for avoiding pills:
“I use herbs more and very little of the medication from doctors. I have faith in the herbs. Pills affect me in a way that makes me afraid to use them.” –An artisanal vendor
Taking into account all the data from interviews and surveys, it is evident that within the mapuche medical system there are treatments for diabetes, hypertension, and cancer. Almost all of the informants were able to ascertain this statement and many could even discuss specific treatments for some of the modern diseases. These treatments are herbal in form, and may prevent, maintain or cure the disease. The extent of the treatment’s effect depends on the stage of advancement of the disease.
“When the machi sees a disease via reading urine, she also knows the advancement of the disease via the spiritual gift that they have. They can see if the disease can be cured with mapuche medicine or if it does not have the ability to be cured with mapuche medicine. So therefore, there are machis that yes, say ‘I can see and treat this disease’ but sometimes they say ‘I cannot see nor treat this disease because it already is very advanced’.” –An intercultural facilitator
Mapuche medicine has been treating and curing wingka diseases since they arrived. Diabetes, for example, is a modern disease that the mapuche identify as “not their own” but can be treated and cured with medicinal herbs and lifestyle changes.
“The mapuche culture can remove diabetes. It removes this, diminishes it, does not increase [the symptoms], they integrate a daily, social activity, that is much more productive. The Mapuche culture, what it does is to take that pattern, that structure and to incorporate it to the society, to valorize it, to increase the use of things that are more healthy for the population. That is what the lonko and machi do through their authority and advising.” –A coordinator of a health care center
However, these types of diseases are still considered modern and therefore their treatment was recently developed within the mapuche culture. The treatments are not ancestral knowledge, rather newly tested applications of the ancient treatment methods.
“At least in the territory where I work, the agents of mapuche medicine are currently testing out alternative treatments for these modern diseases with mapuche medicine. Because don’t forget that these diseases are new. Therefore, since they are new, there is not a very long trajectory in the use of mapuche medicine for these diseases. So there are health agents that are testing, discovering, figuring out if the use of some medicinal herbs can have an effect on healing of these types of diseases. They are not testing out treatments for empacho, or susto, because these are diseases that the people treated since the ancient times and they know perfectly well about the medicine for empacho or susto. Now, for these new diseases there is a certain understanding that these herbs could serve for these diseases. But maybe the characteristics of these diseases suddenly do not allow the herbs to have an effect because there are other factors that influence these diseases.” –Sergio Bermudo Muñoz
Although the interviewees were not able to relay much information about the development process of mapuche treatments for modern diseases, the conversations often naturally transitioned to the causes of these diseases. The perceptions of the mapuche community regarding the cause of we kutran and wingka kutran, focus on the manner in which modernization, urbanization and globalization have changed their cultural traditions, their diet, and their lifestyle. The ancient mapuches mainly gathered fruits, vegetables, and roots. Now the widespread availability of food retracts the need to grow and gather. Nearly all of the informants spoke of the harm of eating refined or processed foods and high amounts of sugar. There is an effort from the mapuche authority figures to recuperate the ancestral diet. A lonko expressed his awareness that the community used to eat a greater amount of vegetables and plants that were medicinal. He explained this concept of food as medicine that is valued within the mapuche culture, “It’s food but also the remedy.” Another informant explained the correlation between diet and efficacy of medical treatment:
“More than just taking medicinal herbs, one also has to eat a medicinal diet. And if there is not a medicinal diet, the medicinal herbs are going to attack the disease very little. So when I give a treatment to a person, there is also a change of their diet. – A lawentuchefe
The ancestral diet as well as natural cultivation methods have all but been forgotten. Many are aware of the visible and invisible damage caused by pesticides, herbicides and chemical fertilizer. Before, the countryside was seen as the sacred mapuche territory. Now it is blemished from the arrival of industrialized food and cultivation techniques, not to mention that mapuche reservations are referred to as “reducciones, “ or “reductions,” since their land was so severely reduced during The Pacification of the Araucanía. Many of the informants also recognized the economic barrier of buying organic, healthy food instead of the widely available processed food. One informant blamed the new free market economy that carried international businesses like Monsanto, international pharmaceutical companies, and toxic food products to Chile. He also identified the loss of cultural identity based on discrimination and shame as a cause of high rates of modern diseases. The concepts of culture, territory, and biodiversity loss greatly affect lifestyle and well-being. Some mapuche individuals believe modern diseases are caused by transgressions made throughout a damaging lifestyle.
“We speak of winka kutran and also we kutran. They are new diseases that the people adopted from a different lifestyle. It’s a lifestyle that is not within the cultural patterns of the cultural formation that we receive. Traditionally, we had our own definitions of what it means to live well. And this we have well forgotten in recent times through contact with immigrants, through internal movement which given the historical situation also moved the native peoples. This is the primary reason that we have adopted new diseases.” –An anthropologist
It is natural that modernization affects cultural values and systems. Although modernity has changed the mapuche medical system, the level of adaptation to the specific mapuche treatments seems miniscule. One informant felt that there have been very few advances in mapuche medicine. This is justified since the methods of machis are ancient and ancestral. In total 4 informants opined that mapuche medicine is the same now as it was before. Five other informants identified small ways in which the mapuche health system has changed. Two informants called the mapuche culture “dynamic” and noted how it incorporated new components. The only specifics given regarding changes to mapuche treatments were concerning the use of non-native herbs for infusions and teas, the use of a cell phone for patient contact, the recommendation to use vitamins, and the availability for a machi to have a high school and undergraduate knowledge. The lack of adaptation of medical treatments was surprising.
“ The machi changes very little. They are using infusions. They don’t introduce many new things. They don’t give pills, nor injections. Nothing more than to have a medicinal drink and cleanse the body.” – A lonko
The only strongly apparent change or variation to the mapuche medical system is its interaction with biomedicine. The single major change to the mapuche medical system is the relocation of their healers from their ancestral land into modern hospitals or health care centers. This phenomena occurred in one of the two investigation sites. The center with machis justified their decision based on an accessibility argument.
“Suddenly mobility, resources, geographic situation has great influence, and this motivated the people to ask to install a [mapuche health] center here. We asked the machis if they can work here, and they said yes. There are some machis that were unable to work here because this depends a lot on their spirituality. If their spirit doesn’t let them come and work in an office, they cannot come. Some can. We have 5 machis that work here. One each day. Here we have two machis that are from the commune of Puerto Saavedra, and the others come from outside.” – A lonko
On the other hand, two other informants were highly vocal about their opposing opinion:
“This link between indigenous medicine and allopathic medicine is not always correct. Because if they try to, for example, take a machi to improve the health problems of the chilean population, I don’t agree. It’s superficial. And it’s functional. The machi is not in culturally adequate, pertinent conditions. Because the role of indigenous health agents is community-based, it’s territory-based, it has to be seen with the greater environment of helping and fixing the conflicts, the relations and how the people come. I question this; up to what point is interculturality going to permit these certain practices or not. We are not visualizing that some day it will explode.” –An anthropologist
“My opinion about a machi in a hospital is that this is the intent to domesticate mapuche medicine. This is so that mapuche medicine can function how the state wants it to function.” –A lonko
The issue of the “modernized” or “sterilized” machi is controversial and highly debated. In each case, the authority figures are attempting to best represent the opinions and desires of their community.
Similarly, very little evidence of medical hybridization in which treatments are borrowed and mixed between two separate medical systems was found. Rather, the mixing of medical systems came from the patients who chose to use different aspects of different medical systems in hopes of healing. This process is classified as medical pluralism instead of hybridism. In this case, treatment methods coexist and are co-utilized but not blended. The medical systems remain distinct entities. As the most frequently discussed topic, there is a plethora of evidence for medical pluralism. This is the main form of adaptation within the mapuche medical system—simply that it is interacting and being utilized with other systems. A lonko justified this plurality by noting that mapuche people move between the mapuche world and the Chilean world so they ought to use both forms of medicine. Many personal histories were given describing their family use of both mapuche medicine and biomedicine. Biomedicine is often only used in extreme cases that are time sensitive or severely advanced. An informant who underwent surgery shared:
“When I had some operations, I took herbs as well. The doctors asked me, ‘Why are you improving so quickly?’ Because I take my herbs and the pills after the operation. I have more faith in the herbal infusions than the pills.” – An artisanal vendor
Many, including the machi herself, mentioned that the mapuche healers may sometimes recommend a patient to see a biomedical practitioner because they know they cannot treat their disease. Diabetes and hypertension were frequently discussed as treatable with mapuche medicine while advanced cancer was often reserved for biomedical treatment.
“There are diseases that are for the doctors. For example, cancer. It is very delicate. As are eye problems, like cataracts. They need operations that I cannot do. In this case, if the disease is so advanced, one is required to tell the patient to go to the hospital.” – A machi
When the machi reads urine, it shows her whether or not the disease can be treated with mapuche medicine and which herbs to use if the treatment is viable. Moreover, those familiar with the Mapuche Health Care Center in Puerto Saavedra considered both medical systems valuable and encouraged patients to utilize both the hospital and the mapuche center as they choose. There was an obvious avoidance of discussing one system as better and the other as worse from all the informants. However, an interesting relationship between simplicity of the disease and viability of mapuche medicine was found.
“If the disease is serious, they can use pharmaceuticals, but for simple illnesses or for prevention, we treat with home remedies. We also treat with diet, organic food. But when a disease comes, if it’s very serious, obviously I’m going to take medication from the doctors, possibly surgery.”–A social worker
All those with mapuche background were willing to embrace medical pluralism. Unfortunately, it is possible that the dominant biomedical system is unable to fully embrace this coexistence and co-utilization of medical practices, thus perpetually subjugating mapuche medical system as an “alternative” or “complementary” medicine.
I think that it comes more from the indigenous world or from the mapuche medicine, where the agents of mapuche health or the users or the patients, apart from their herbs they also take western medicine. But it is more an initiative from them. Or because someone says to them look, apart from the medication that you get from the health post, also use these herbs. But these indications come from the family or from the lawentuchefe or from the machi but western health professionals don’t have the same attitude. It’s rare that a doctor is going to say, ‘together with the medication, use herbs.’ It’s not very common that someone from western medicine makes this suggestion to use the two types of treatments. The people use it on their own initiative because deep down they are asking, how are they going to improve their health condition, how can they stop the ailments, then they investigate, seek, ask and use the two types of medicines. It is not because the health agents of our system have the intercultural initiative not to prescribe, but to recognize and support the work of the patient, to respect those who use Mapuche medicine. I’ve never heard of this exception. But there are some exceptions. For example, we have received information that specialist doctors suddenly have a different view and more ability of strengthening mapuche medicine than the primary care physicians themselves. But primary care doctors have more contact with the community, they converse with the people, so they should support and incentivize the use of mapuche medicine. At least from what we’re familiar with, this isn’t happening. It is occurring on the specialization level. – Sergio Bermudo Muñoz
Regarding this subjugated classification as “alternative” or “complementary,” the informants almost unanimously feel that their medical system is self-sustaining, independently valuable, and does not need to merely act as a “complement” to biomedicine. Four informants mentioned the Law of Patient Rights, but one felt that even the formation of the law was insufficient in acknowledging mapuche medicine as equivalently important.
“The law of the rights and duties of patients incorporate in its article 7, the cultural relevance of care. But it itself is a contradiction. Because cultural belonging is a right won by peoples. This is one of the main differences with other segments of the population. The indigenous are put in the sack of the excluded. It’s like alternative medicine or alternative populations. We enter with the ‘other’.”–An anthropologist
Mapuche medicine should coexist with biomedicine and other ethnomedical systems. Furthermore, the medical systems should be able to converse, to share knowledge and develop mutual respect. The “other” medical systems should not only be recognized, but recognized as valuable and effective in their own ways. It seems this barrier has yet to be overcome.
“I’m going to talk about my experience in Santiago. An almost generalized ignorance exists regarding mapuche medicine. Some elements are known very superficially and it is obvious that they are not considered, not valued, not realized, not recommended. I think that all this happens because one is not familiar with the system, and because of the history and also the myths. It is seen as something that is not valued, as something popular, something like a home remedy, of lower level and lower quality. They see it as something that cannot be part of their process or of formal, institutionalized treatment. Now, yes, there are some approaches of some people who have a little more openness towards the subject, but I don’t think it is valued from the health professionals and the formal practitioners despite the programs that are in place, despite the “advancements”. At least in the city, it is not considered as a medical system, it is not a possibility. They think mapuche medicine comes from a point a view that is more ludicrous, more folkloric. I think this is a theme of ignorance as well that they don’t have education about cultural competence. They will never talk about it either. This is a transversal issue of education of the process of the mapuche people and their knowledge. It’s a cultural clash. It’s a political theme. The doctors say, ‘Ah, yes we talk about interculturality, of indigenous peoples, of migrants.’ It’s only something superficial, something pretty, something to serve for the photos. I at least perceive this. –An intercultural facilitator
These sentiments from biomedical professionals are systemic in nature. They start with primary education where science is taught as the superior system, inseparable from medicine and healing:
“Currently, the biomedical system is based on scientific evidence. If it’s not shown, it doesn’t exist. This is like not being able to think in other forms of doing medicine that don’t necessarily have scientific evidence. Even when we say, yes, there is scientific evidence because mapuche medicine is ancestral. It still survives until this moment and has healed many people. However, from the mapuche community it is not important to have the evidence that biomedicine has. So of course, there are elements that obviously subordinate not only the mapuche knowledge but also the popular knowledge and other cultures, home remedies for example, all of this that is not considered within the scientific possibility to cure”. –An intercultural facilitator
Even in medical school, doctors are not sufficiently taught about sociocultural and anthropological issues due to a lack of time. And if there is cultural education, the mapuche find it too superficial.
“Not all of the doctors understand the form of mapuche medicine. Very few are interested. But the majority are not. Or if they know, it is very superficial. Sometimes they participate in activities like we tripantu, but they still lack the desire to have a deeper conversation”. –A lonko
Discussion and Conclusions
First, it is important to realize that not all of the research objectives were completely obtained and this is perfectly acceptable. The study unexpectedly made interesting findings regarding the mapuche medical system and the process of modernization of the culture. However, the process of modernization/adaptation of medical treatments within the mapuche medical system was not completely characterized because there was not much discourse of the changes to specific treatments. In fact, many of the informants spoke about the lack of adaptation to mapuche treatments; the machis are still using herbal infusions and spiritual ceremonies as before. Although various parts of the mapuche culture have been lost through modernization, the treatment methods are maintained. Regarding the spiritual aspect of mapuche medicine, it seems that medicinal herbs are currently utilized much more frequently than spiritual ceremonies as treatment.
Attempting to understand how traditional treatments were developed for chronic non-transmittable diseases like we kutran and wingka kutran proved to be difficult. Therefore, the study obtained very little information regarding this issue. The only strong data on the development of treatment for modern diseases is that mapuche health agents are still testing and experimenting with the herbs that are currently accessible. The difficulty of obtaining this information can be attributed to the lack of access to machis for interviews. Of course, machis would know best how treatments were developed, but because of the short length of the study, it was not possible to make the long-term friendly relationships with the machis needed to discuss these issues. And even if a machi was found that was very willing to talk and very open, it is possible that she could not share her knowledge of the treatments because her spirit does not allow this type of transmission to foreigners, especially a person without a spiritual gift like theirs.
As for why the treatment developed for modern diseases within mapuche medicine, informants spoke mostly about the cause of modern diseases that affect mapuche people. The conversation almost always transitioned to a discussion about diet and agriculture. The free market and the loss of culture, identity, and biodiversity were also mentioned as reasons for the arrival of modern diseases in the Mapuche community.
Regarding treatment of modern diseases, the high presence of medical pluralism and the lack of medical hybridization manifested as key findings. Mapuche citizens and mapuche health agents are obviously pluralistic in their treatment of modern diseases, using their own system as much as biomedicine and other ethnomedical treatments and home remedies. But it seems that the world of biomedicine cannot accept this reality.
Indigenous peoples find mapuche treatment to be as important and valuable as biomedical treatments for modern diseases. They respect both systems for their capabilities and deficiencies. Many informants feel that cancer is a modern disease for which biomedical treatment is very useful and necessary. But for diabetes and hypertension, they think that mapuche medicine can treat, maintain or cure these diseases with healthy and ancestral food, herbs from a machi or lawentuchefe, and by following the patterns of good life of the mapuches.
Some modern diseases have a name in mapuzungun, but it is rarely used. Still, they are interpreted as “not our own” to the mapuche culture. These diseases are not understood as spiritual, so they typically do not perform a spiritual ceremony to cleanse the body of diabetes or hypertension.
The surveys show that the preference of the mapuche community for their treatment is highly variable. Some use mapuche medicine occasionally or exclusively, but others never use it. But many of the informants agree that the biomedical system does not recognize or respect their form of medicine very well.
The biggest unexpected finding is that the main way mapuche medicine has adapted is simply its interaction with biomedicine and modern infrastructure. Recently, machis are working in a hospital or health center. This is the most significant change to mapuche medicine and it is not without debate.
It was concluded that it is necessary to test the methods of a study in a preliminary manner and to expect changes to the design of surveys and interviews because each population is unique and responds in different ways. It was also concluded that the duration of the study was too short to be correctly conducted. The mapuche are very aware of colonialism because of their history. For this reason, the intention of the collection of information was constantly justified but sometimes not enough.
More time is recommended to do the project, or at least more time to plan the design before executing the study. Or rather, investigators are encouraged to form a community partnership where the work can be more profound and reciprocal. Further research should study how the aspects of mapuche medicine were maintained and why this part of their culture escaped dramatic change.
Biomedical health professionals are advised to realize that although biomedicine is very useful and very important to our society, other forms of health care are equally useful in their own ways, and that patients will use any kind of treatment that they believe will work for themselves.
Limitations
The language barrier contributed the biggest limitation of the study. Communication with citizens for surveys was especially difficult. Furthermore, some interviews and surveys were time-restricted based on the informant’s availability, making profundity of investigation difficult. Finally, the entire project was extremely restricted in the length of study. The one month time frame in which one had to design the study, make contacts, complete interviews and surveys and finally summarize, analyze, and discuss the project was entirely too short. The investigator negotiated the intention of the project on several occasions with informants, frequently weighing anthropological ethics and the obligation to complete the assigned project. Considering the sensitivity of this sort of anthropological study, one can conclude that this hyphenated investigation period ought to be revised if similar studies are to be replicated. The inability to form a priori relationships not only burdened the informants but also the entire investigation’s purpose. It has been confirmed that this sort of cultural sharing requires long-term relationship formation. This region was chosen for the investigation due to the admiration of the strength and resistance of the mapuche community. It feels unjust to extract their information for the benefit of a U.S. American student in the very colonial manner that they have resisted for centuries. For this reason, it is imperative to make findings available to both the U.S. American and Chilean public. I recommend that in the future, these studies are built into community-based internships or volunteer work that do in fact empower the community being studied.
References
Awah, P. K., & Phillimore, P. (2008). Diabetes, medicine and modernity in Cameroon. Africa, 78(04), 475-495.
Bacigalupo, A. M. (1993). Variación del rol de machi dentro de la cultura mapuche: tipología geográfica, adaptiva e iniciática. Revista Chilena de Antropología, (12).
Bosio, C., Tomasoni, G., Martínez, R., Olea, A. F., Carrasco, H., & Villena, J. (2015). Cytotoxic and apoptotic effects of leptocarpin, a plant-derived sesquiterpene lactone, on human cancer cell lines. Chemico-biological interactions, 242, 415-421.
Caniullan Victor. (2017). Mapuche Lawentuwün Sugu [PPT]. SIT World Learning,
“Salud Pública, Medicina Tradicional y Empoderamiento de la Comunidad”, Arica, Chile.
Cuyul, Andres (2017). Procesos socioculturales y salud [PPT]. SIT World Learning, “Salud Pública, Medicina Tradicional y Empoderamiento de la Comunidad”, Arica, Chile.
Cuyul, A. (2012). Salud intercultural y la patrimonialización de la salud Mapuche en Chile. Ta iñfijkexiparakizuameluwün. Historia, colonialismo y Resistencia desde el País Mapuche, 263-284.
Colicoy, Domingo (2017). Mapuche, Kvñen Mapu Caijiwe Comuna de Nueva Imperial
PPT]. SIT World Learning, “Salud Pública, Medicina Tradicional y Empoderamiento de la Comunidad”, Arica, Chile.
Johnson, Brian (2017). Información Población Indígena en Chile. Viaje de Campo La Araucanía. P. 12
Menéndez, E. L. (2005). Intencionalidad, experiencia y función: la articulación de los saberes médicos/Intention, experience and function: articulation of medical knowledge. Revista de antropología social, 14, 33-71.
Montenegro, R. A., & Stephens, C. (2006). Indigenous health in Latin America and the Caribbean. The Lancet, 367(9525), 1859-1869.
Muñoz, S. H. B. (2016). Understanding Mapuche-Williche Conceptions of Diabetes Mellitus and Arterial Hypertension from the Perspective of Intercultural Health. Social Medicine, 10(3), 83-92.
Muñoz, S. H. B (2015). Río Chuelo, Espacion de pensamientos y saberes en salud intercultural.
Pedrero Sanhue, Malva-marina (2011). Perfil epidemiológico básico de la población mapuche residente en el área de cobertura del Servicio de Salud Osorno. Ministerio de Salud (52-59).
Pichinao, Jimena, Ernesto Huenchulaf, y Fresia Mellico (2003). “Pu Mapunche ñi Gijañmawün”: La forma mapuche de hacer religión. Informe inédito para la COTAM
Torri, M. C. (2011). Illness and Healing in Urban Areas in Chile: Between Tradition and Cultural Adaptation. Oxford Development Studies, 39(4), 389-402.
Torri, M. C., & Laplante, J. (2013). Traditional Medicine and Biomedicine among Mapuche Communities in Temuco, Chile: New Forms of Medical Pluralism in Health Care Delivery. Anthropologica, 413-423.
Image: pxhere.com
