

By Rosalie Mattiola
The following text is an excerpt from a research paper written in spring 2017. To read the full text and to see the sources used, click here.
Introduction
Mortality
Between 1997 and 2013, Chile experienced a shift in mortality rates of diseases considered “modern” or “western” like cancer, diabetes and cardiovascular disease. The number of deaths caused by malignant tumors of the colon, sigmoid, rectum, anus, liver, pancreas, trachea, bronchus, lung, head, lymphatic tissues, hypertensive disease, cardiac arrhythmias, arteriosclerosis, aneurisms, and aortic dissections have dramatically increased in the last two decades. Within 16 years, the number of deaths from cancer of the colon, sigmoid, rectum, anus, pancreas, trachea, bronchus, lung, and head have more than doubled. Those caused by hypertension jumped from 1,700 in 1997 to 4,574 in 2013. Moreover, the number of deaths from cardiac arrhythmia more than tripled in this time (DIES-MINSAL Series Principales causas de muerte tasas según sexo Chile).
In the region of Araucania, where the highest percentage of indigenous peoples reside (Johnson 2017), the mortality rates for malignant tumors increased from 123.1 to 153.2 deaths per 100,000 habitants over the period of 2000 to 2011 and that of hypertensive diseases increased from 12.5 to 20.7 deaths per 100,000 inhabitants (DIES-MINSAL Series 11- Araucania). The death rate from diabetes remained level but the UN Report on the Health Status of the World’s Indigenous Populations highlighted alarming rates of diabetes: “Worldwide over half of indigenous adults over 35 have type II diabetes. These numbers are expected to increase. In some indigenous communities, diabetes has reached epidemic proportions and has threatened the very existence of the community” (Muñoz 2016).
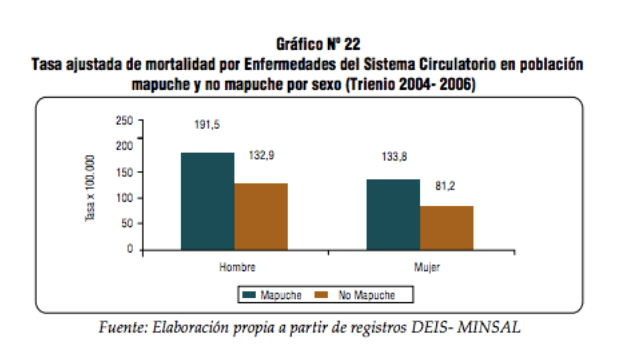
Within Araucania, it has been found that indigenous inhabitants are subject to higher mortality rates for the same diseases than compared to the non-indigenous Chilean citizens. The Ministerio de Salud (Ministry of Health) presents data showing the mapuche indigenous population to have a 60% higher risk of dying from illnesses of the circulatory system than non-mapuches (Pedero Sanhue 2011).
Mapuches in urban settings almost always have a much higher mortality rate than those in rural areas (Pedero Sanhue 2011). The same concept holds true for mortality by cerebrovascular disease and cancer, although the mapuche burden of cancer mortality is stronger amongst females than males.
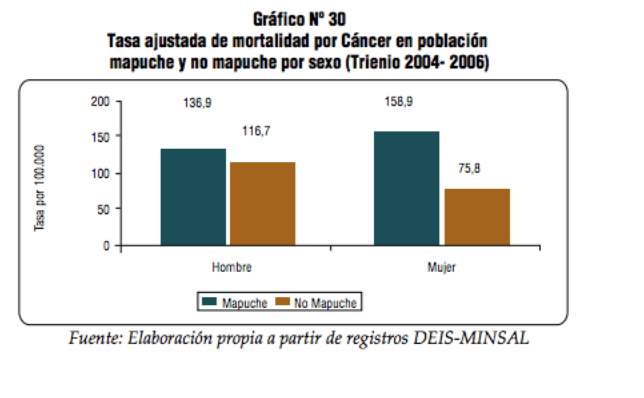
The mortality rate of cancer of the digestive organs in mapuche women is especially alarming.
Modernity
The appearance of the aforementioned modern diseases amongst Chileans and mapuches can be associated with modernization over the last three decades. Muñoz defines the concept, citing Bengoa (1996:7): “Modernization, understood as the uncritical adoption of norms, behaviors, and products coming from “developed” countries, is now a universal reality” (2016). New lifestyles, diseases, systems of health care and treatment methods have mixed within the indigenous culture. A common trait of modernization of indigenous communities is the increased vulnerability to “modern” diseases, which is widely affected by social determinants of health (Montenegro 2006). Linking modernization to urbanization and transfer of knowledge, Torri explains, “with the process of increasing assimilation to the dominant Chilean culture following immigration into urban areas, the Mapuche are exposed to new concepts when chronic illnesses, such as cancer, stroke and diabetes, are diagnosed by biomedical practitioners” (2011). The diseases diagnosed by biomedical practitioners are then interpreted, rationalized and treated by the mapuches. A study from Muñoz found that “All users identified diabetes and hypertension as diseases ‘that we didn’t have previously.’ They attributed these diseases to the consumption of processed foods with high fat and sugar content and associate these foods with a modern lifestyle” (2016). Therefore, modernity has had a visible effect on the health of the indigenous.
It is important to note that the labeling of ideas and concepts as “modern” forces the presence of the opposing label “unmodern.” The current hegemonic system assigns value to the concept “modern” and undermines all things “pre-modern” (Awah 2008). This project attempts to avoid this designation of “better” or “worse” associated with modernity. When methods and beliefs adapt, it is not because they are seeking to become more modern and thus better, rather that they change to meet the need of the community. This change is inevitable when confronted with modernization. “Modern” and “pre-modern” concepts cross and interact. Modern diseases are not only knowable by modern medicine—it is permissible and acceptable for modern diseases to be treated by unmodern medicine (Awah 2008). This is precisely what this investigation seeks to study—the intersection of modern and unmodern and the adaptation of practices based on the transmission of knowledge.
Image: pxhere.com
Rosalie Mattiola is a student at George Washington University.
